
- Why Deep Neck Anatomy Matters In Neck Contouring Surgery
- Take The Quiz
- The Superficial Layer – Skin, Fascia And Platysma Muscle
- Download Dr Kernohan’s Facelift Surgery Guide
- Intermediate Structures – Platysma, Retaining Ligaments And Interplatysmal Fat
- Deep Neck Components in Neck Contouring Surgery – Subplatysmal Fat, Digastric Muscles And Glandular Structures
- Fascial Planes And Their Surgical Implications
- How Age‑Related Changes Affect Neck Shape
- Platysma In Detail – Function, Innervation And Surgical Considerations
- The Digastric Muscles And Cervicomental Contour
- Deep Fat Compartments: Supraplatysmal And Subplatysmal Layers
- Surgical Implications – Planning For Deep Plane Neck Contouring
- Facelift Before and After Photos
- Individual Variation In Neck Anatomy
- Looking Forward: A Deep Approach to Optimal Neck Contour
- Deep Neck Anatomy And Neck Contouring Surgery FAQs
- Next Step: Book A Personalised Neck Assessment With Dr Michael Kernohan
- Further Reading
Why Deep Neck Anatomy Matters In Neck Contouring Surgery
A well-defined and balanced neck can play an important role in overall facial proportion. Planning surgery in this area, whether as a neck lift surgery in Sydney on its own or together with facial surgery, involves understanding the deeper structures beneath the skin. These include muscle layers, fat layers, fascial planes, and bony landmarks, which together influence neck shape, support, and movement.
Dr Michael Kernohan, Specialist Plastic & Reconstructive Surgeon in Sydney, emphasises that effective neck contouring goes beyond skin tightening. Expert surgeons assess and work with deeper structures such as the platysma muscle, digastric muscles, and the deep fat compartments to create optimal results and avoid common postoperative issues. Recognising how each layer contributes to neck shape, supports both safer surgical planning and more consistent outcomes.
This article explores these anatomical features in depth, discusses how they influence neck ageing and shape, and explains how surgeons integrate this knowledge into personalised surgical strategies. A deeper anatomical understanding also helps patients make informed choices about surgical options and anticipated results.
Take The Quiz
The Superficial Layer – Skin, Fascia And Platysma Muscle
The most visible part of the neck is the skin and subcutaneous tissue, but just beneath the surface lies a thin yet functionally significant muscle called the platysma. The platysma lies within the superficial cervical fascia, a layer of connective tissue just under the skin that also contains superficial nerves, veins, lymphatics, and fat.
The platysma is a broad, thin muscle that originates from fascia in the chest and shoulder region, then ascends medially across the front and sides of the neck to insert around the lower mandible, lower face and lips. Its fibres interlace in the midline and contribute to facial expression by helping depress the jaw and lower lip, and they also influence how the skin moves and folds across the neck.
Because the platysma lies so superficially, changes in its tone or position significantly affect neck appearance. With ageing, the muscle’s fibres can separate or weaken, leading to vertical bands and loss of smooth contour. Proper surgical understanding of this layer helps surgeons address these dynamic features appropriately during a neck lift surgery.
Download Dr Kernohan’s Facelift Surgery Guide

Intermediate Structures – Platysma, Retaining Ligaments And Interplatysmal Fat
Beneath the skin and superficial fascia, the neck’s intermediate layer consists of the platysma muscle, interplatysmal fat, and supportive ligamentous structures. This layer plays a central role in how the neck contour changes with age. In classic descriptions of neck anatomy, the superficial layer is distinguished from deeper compartments by the presence of the platysma and the fat immediately beneath it.
The interplatysmal fat lies between the two platysma muscle sheets and can accumulate or shift with age, creating fullness or irregular contouring along the anterior neck. Retaining ligaments and fascial connections help anchor the platysma to deeper tissues; when these structures weaken, the platysma can separate medially, contributing to characteristic “platysmal banding.”
Surgeons use this layered perspective to decide how much of the platysma and interplatysmal fat to address during a neck lift. Decisions about muscle plication, selective fat removal, or fascia release are influenced by how these intermediate elements interact with the surrounding anatomy.
Deep Neck Components in Neck Contouring Surgery – Subplatysmal Fat, Digastric Muscles And Glandular Structures
Below the platysma and interplatysmal fat lies the deep plane of the neck, which includes subplatysmal fat, the digastric muscles, the submandibular glands, and the skeletal support provided by the hyoid bone and mandible.
The deep fat compartments are anatomically distinct and often defined in cadaver studies. One analysis showed that supraplatysmal fat (above the platysma) represents about 44.7 % of neck fat, while subplatysmal fat deep to the muscle accounts for another 30.7 %, with small amounts of deeper fat adjacent to glands and other structures.
The digastric muscles, situated inferior to the mandible and deep to the platysma, play a role in defining the cervicomental angle – the curvature between the underside of the chin and the neck’s anterior surface. Submandibular glands also contribute to contour beneath the jaw; when prominent or ptotic, they can obscure underlying definition even when skin and muscle tone are addressed.
Fascial Planes And Their Surgical Implications
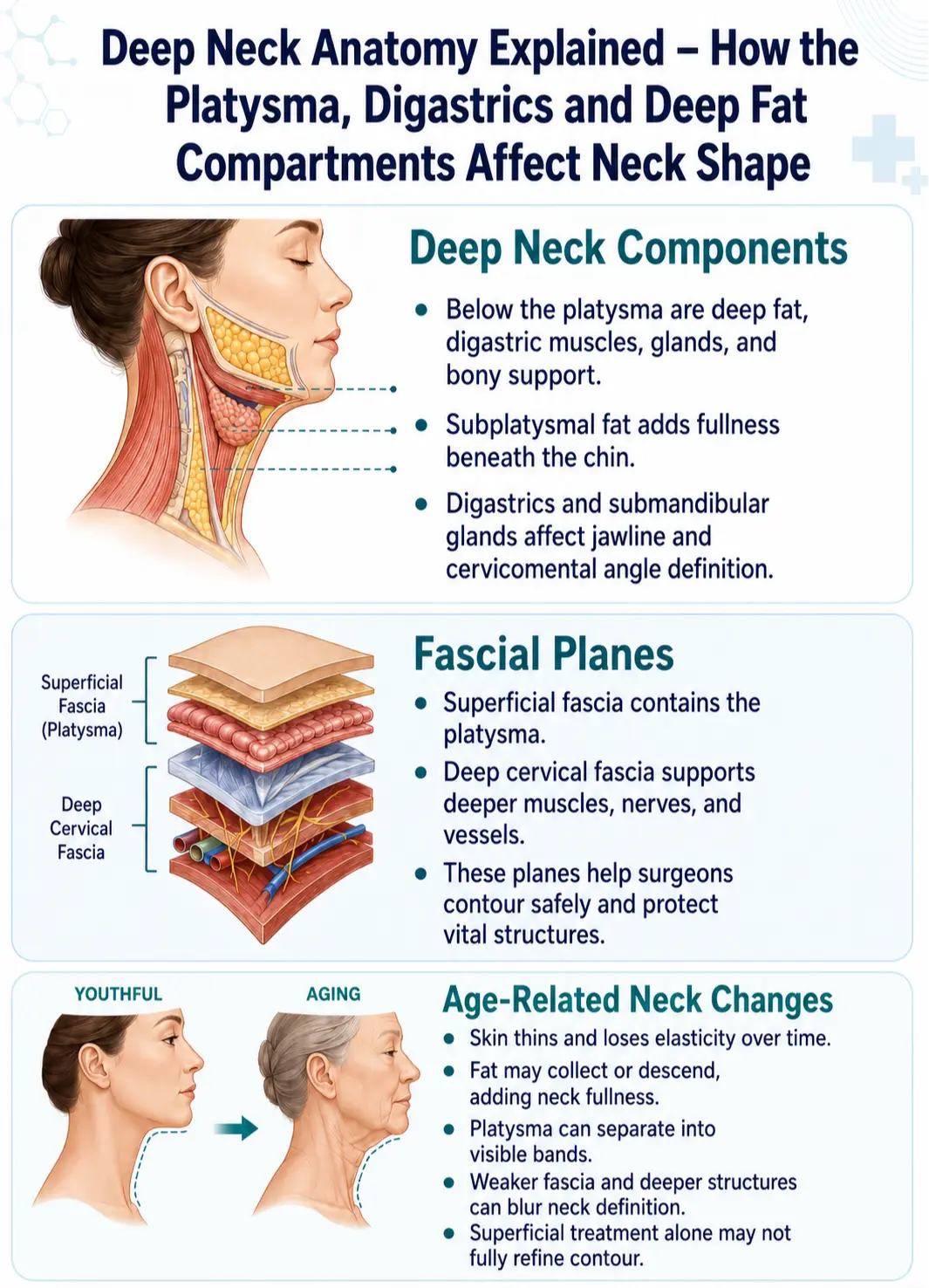
The neck’s fascial architecture consists of multiple layers that organise and compartmentalise structures. The superficial cervical fascia contains the platysma, while the deep cervical fascia has several subdivisions – investing, pretracheal, and prevertebral – that support deeper muscles, viscera, vessels, and nerves.
These fascial layers allow tissues to slide and move relative to one another, which is important during swallowing, head movement, and neck surgery. Surgeons rely on this anatomical arrangement to develop surgical planes safely, avoid vital structures, and reposition tissues in a way that supports both contour and function.
Understanding fascia is also critical in procedures that involve deeper dissection, such as deep‑plane neck lifts or techniques that address subplatysmal fat and digastric influences. Safe navigation of fascia minimises risks to nerves, blood vessels, and glandular structures while maximising contour refinement.
How Age‑Related Changes Affect Neck Shape
As the neck ages, several anatomical changes occur simultaneously. The skin becomes thinner and loses elasticity, reducing its ability to recoil after movement or stress. Subcutaneous and deeper fat compartments may accumulate or descend, contributing to fullness under the chin or along the jowl line.
The platysma muscle’s fibres can separate or weaken, creating vertical ridges or bands that are visible even at rest or when talking. At the same time, ligaments and fascial structures lose tension, which allows deeper tissues such as subplatysmal fat to protrude, obscuring the natural cervicomental angle. In some individuals, the anatomy of the digastric muscles or submandibular glands contributes to a convex neck profile, making contours less defined.
Together, these age‑associated patterns explain why a superficial approach – addressing only skin and subcutaneous fat – is often insufficient for achieving a refined neck contour in many patients.
Platysma In Detail – Function, Innervation And Surgical Considerations
The platysma is a broad, thin sheet‑like muscle that covers the anterior and lateral neck and is innervated by the cervical branch of the facial nerve (cranial nerve VII). Its fibres originate from fascia over the clavicle and shoulder regions and ascend to insert into the mandible, lower face and muscles of facial expression.
Beyond its cosmetic implications, the platysma plays a role in expression – tightening the neck’s surface and contributing to movements of the lower lip and jaw. Because it lies directly beneath the superficial fascia, it is also an important landmark in surgical dissection, and careful handling is essential to preserve nerve supply and avoid functional deficits.
Changes in its anatomical arrangement, such as medial separation or detachment with age, contribute to banding and contour irregularities. Techniques such as corset platysmaplasty or advanced plication aim to unify and reinforce this muscle sheet, reducing the appearance of bands and improving contour.
The Digastric Muscles And Cervicomental Contour
The digastric muscles are two‑bellied muscles that lie deep to the platysma and contribute to the anterior neck architecture. They attach near the mandible and hyoid bone and help define the submental contour and cervicomental angle.
The anterior bellies of the digastric muscles border the submental space, a fascial region beneath the chin that surgeons often reference when planning neck lift dissection or fat removal. Prominence or ptosis of these muscles can contribute to an unrefined neck contour even when subcutaneous and surface features are improved, which is why some advanced techniques address their influence directly.
Addressing deep elements like digastric muscle influence may involve selective myotomies or fascial releases as part of a comprehensive contouring strategy in suitable candidates.
Deep Fat Compartments: Supraplatysmal And Subplatysmal Layers
The neck’s fat is not uniform but compartmentalised into distinct layers with different surgical implications. Supraplatysmal fat lies above the platysma and blends with subcutaneous tissue, contributing to surface fullness.
Below the muscle, subplatysmal fat sits between the medial edges of the anterior digastric muscles, and it can be a major contributor to deeper convexity in the upper neck. These deeper fat pockets require careful assessment because simple liposuction of the superficial layer may not sufficiently refine contour if subplatysmal fat remains. Surgeons often distinguish between these layers during planning to tailor fat removal and contouring accurately.
Surgical Implications – Planning For Deep Plane Neck Contouring
Working with the deeper structures of the neck requires both anatomical precision and clinical judgement. Surgeons must determine whether a superficial lift, submental liposuction, or full deep plane neck contouring is necessary based on the specific combination of fat, muscle, glandular, and fascial contributions to neck shape.
Procedures that involve subplatysmal fat removal, digastric muscle reduction, or submandibular gland reshaping are generally considered more advanced. They carry a slightly higher level of complexity and are not necessary for every patient. However, in individuals with prominent deep neck fullness or recurrent banding after a previous surgery, they may be the key to achieving lasting contour.
Dr Michael Kernohan, Specialist Plastic & Reconstructive Surgeon in Sydney, incorporates these deeper considerations into his surgical assessments. By evaluating deep fat distribution, muscular dynamics, and fascial balance, he can recommend a surgical approach that is comprehensive yet tailored – preserving form and function while enhancing definition.
Facelift Before and After Photos


Disclaimer: All surgical or invasive procedures come with inherent risks, and results can vary widely between individuals due to factors like lifestyle, anatomy, overall health, weight, and nutrition. We encourage you to conduct thorough research and consider seeking a second opinion from a qualified healthcare provider.
Individual Variation In Neck Anatomy
It’s important to note that deep neck anatomy varies considerably among patients. Factors such as weight, genetics, posture, previous procedures, and age can influence the size, shape, and positioning of muscles and fat compartments. Additionally, skeletal landmarks like mandibular projection and hyoid bone height affect neck angle and definition.
Some patients have prominent submandibular glands that are visible even in youth, while others accumulate deeper fat with age. In other individuals, digastric muscle positioning or tension creates anterior neck fullness that cannot be resolved with superficial techniques alone.
For these reasons, a one-size-fits-all approach to neck contouring is rarely effective. A thorough anatomical assessment that includes surface inspection and, in some cases, imaging, allows the surgeon to identify what structures are most responsible for a patient’s concerns – and to avoid unnecessary or ineffective interventions.
Looking Forward: A Deep Approach to Optimal Neck Contour
Achieving optimal neck contour through surgery is about more than skin tightening. It requires an understanding of the layered architecture beneath the surface – especially the platysma muscle, digastric influences, and deep fat compartments. These structures affect both static and dynamic neck appearance and require tailored management depending on each individual’s anatomy.
Surgeons like Dr Michael Kernohan, with extensive experience in reconstructive anatomy and facial surgery, use this deep anatomical insight to provide safer, more effective and longer-lasting outcomes. His clinic in Sydney offers a thorough evaluation process that takes into account both superficial and deep features to determine the right approach for each patient.
For those considering a neck lift, particularly patients who’ve noticed persistent fullness, banding, or lack of definition, understanding the role of deep neck anatomy is a valuable first step in seeking a solution that fits your goals and unique anatomy.

Deep Neck Anatomy And Neck Contouring Surgery FAQs
Next Step: Book A Personalised Neck Assessment With Dr Michael Kernohan
If you’re considering neck surgery and want to explore how deeper structures like the platysma, digastrics, or subplatysmal fat may be influencing your results, you may consider booking a consultation. Dr Michael Kernohan, Specialist Plastic & Reconstructive Surgeon in Sydney, takes a layered anatomical approach to neck assessment and surgery – ensuring that each treatment plan is customised to your facial structure, tissue depth, and long-term goals.
Start with a confidential consultation or submit your photos online for an expert surgical opinion. The path to a more refined, anatomically tailored outcome begins with understanding the structures that make up your unique neck contour.
Further Reading
- Read more about Partial Neck Lift Sydney
- Read more about Neck Lift Recovery Tips for a Better Result
- Read Dr Kernohan’s Blog on Should You Trim Glands During A Neck Lift?
- Read Dr Kernohan’s Blog on Exercise After a Neck Lift for Excess Skin Removal
- Read Dr Kernohan’s Blog on Neck Lift Options – Types of Neck Lift Surgery
- Read Dr Kernohan’s Blog on Managing and Treating Necklift Scars
- Can A Neck Lift Be Done Without A Facelift?

High-SMAS vs Deep-Plane Approaches in Neck Lift Surgery
Why Technique Matters In Neck Lift Surgery When planning a neck lift – especially in…
Incisions in a Neck Lift – Where They Are Placed and Why
When people start looking into neck lift surgery, one of the most common questions is,…

How Weight Changes Affect Neck Appearance
Many people in their 40s, 50s and 60s notice the same thing in photos: even…



